
The 6 most important things to remember when working with Vestibular Dysfunction:
- 1 – Vestibular dysfunction is more common than you think
In 2009, Agrawal et al published a great article: “Disorders of Balance and Vestibular Function in US Adults” So, what was the result of the study? Let’s sum it up:
- “The prevalence of vestibular dysfunction in the US population aged 40 years and older from 2001-2004 was 35.4%.”1
- The prevalence of vestibular dysfunction increased markedly with age
- 85% of individuals age 80 and above had evidence of vestibular/balance dysfunction2
- Higher prevalence rates of vestibular dysfunction were found in individuals with cardiovascular risk characteristics such as:1
- Heavy tobacco use (≥20 years)
- Hypertension
- Diabetes
- The odds of balance dysfunction were found to be 70% higher among individuals with diabetes mellitus2
So, approximately 35% of the US population 40 years and older have some sort of vestibular dysfunction. Then as we age, there is a significant increase in the likelihood of developing vestibular dysfunction. By 80 years and older, 85% of that population has evidence of vestibular and balance issues! That may give some insight as to nearly 1 in 4 people over 65 fall each year.3
Recognizing when vestibular dysfunction is present and addressing the symptoms may help someone reduce their risk of falling. In another study, approximately 1 in 10 individuals in an urban community setting have undiagnosed Benign Paroxysmal Positional Vertigo.5 Maybe you should rethink if orthostatic hypotension really is the reason why your patient felt a little dizzy when sitting up from the plinth or treatment table! You don’t have to be in a neuro clinic or be a vestibular therapist to be in the presence of BPPV or unilateral hypofunction.
- 2 – There is more than 1 canal in the vestibular system
It is very common for a patient to be tested for BPPV with a Dix-Hallpike, and then assumed to be a positive test if the patient’s symptoms are recreated. That may not always be the case! Yes, posterior canal BPPV is the most common canal involved, but there is also the horizontal canal and the anterior canal. The posterior canal is involved in 80% of cases, the horizontal canal in 15%, and the rarest form of BPPV (5%) is in the anterior.4 We have to watch for the eye movements that are associated with the canal you are testing. Here’s an example of a patient who doesn’t present with the torsional up-beating nystagmus associated with the posterior canal. Her strong horizontal nystagmus indicates that the BPPV is in the horizontal canal.
- 3 – There is more than a Dix-Hallpike Test
If you just want to keep things quick and simple, screening for BPPV or possible unilateral hypofunction is easy and doesn’t require any equipment. First assess ocular motility and smooth pursuits. Then perform a head thrust test. Finally, perform a Dix-Hallpike (posterior canal BPPV) and Roll Test (horizontal canal BPPV). These tests should ideally take less than 10 minutes, and may give you a hint as to why a patient may feel dizzy and imbalanced. Tada! You’ve just completed a simple mini bedside examination.
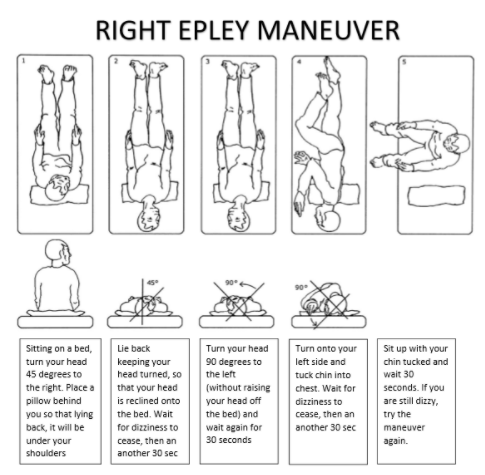
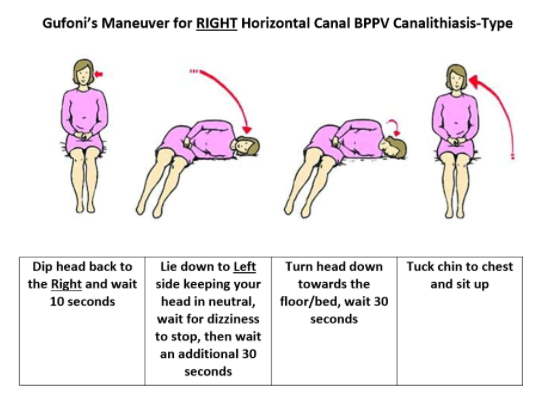
- 4 – There is more than an Epley
In the case of the video shown above, the patient endured many unsuccessful Epley maneuvers… mainly because her problem was in the horizontal canal, not the posterior. Misdiagnosis of the location of the displaced crystals/otoconia can result in further complications and development of other conditions that are harder to treat such as cupulolithiasis and a canalith jam. Not to mention, this patient was terrified of her vertigo, and has developed a lot of anxiety. Her life was greatly altered by her condition. There are many different types of treatments, but in the intrest of simplicity: Epleys are great for posterior canal BPPV, and modified Gufonis are effective for horizontal canal BPPV (canalithiasis). Here are two examples of each maneuver:
- 5 – All you need is Ewald’s Laws and your two hands!
If you can remember Ewald’s Laws, and that nystagmus always beats to the more neurally active ear (excited ear), then you can easily picture what is going on in the Dix-Hallpike and Roll tests:
- First Law: The direction of the nystagmus is directly correlated to the canal that is being stimulated… not the position of the head.
- Second Law: Fluid flow (or otoconia) moving towards the cupula in the HORIZONTAL canal is an EXCITATORY stimulus.
- Third Law: Fluid flow (or otoconia) moving away from the cupula in the VERTICAL (posterior and superior/anterior) canals is an EXCITATORY stimulus.
Be sure to review your vestibular anatomy!
- 6 – It (usually) doesn’t hurt to try
Okay, so vestibular testing and therapy can be a little confusing, I know. However, most of the time, it does not hurt to at least try to help a patient. As mentioned before, 80% of BPPV cases are in the posterior canal. If you perform your Dix-Hallpike, and have determined the side involved, at least try the Epley! Youtube it if you’re desperate. As physical therapists (quoting the APTA), it is our job as “licensed health care professionals [to] help patients reduce pain and improve or restore mobility – in many cases without expensive surgery and often reducing the need for long-term use of prescription medications and their side effects.” If you are uncomfortable with examination and treatment, have a list handy of people whom you can refer the patient to for help. A great resource can be found on the website for the Vestibular Disorders Association (www.vestibular.org). There, you can search for providers in your area who specialize in vestibular examination and treatment.
References:
- Agrawal Y, Carey JP, et al. Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001–2004. Arch Intern Med. 2009;169(10):938–944. (http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/773517)
- Agrawal Y, Carey JP, Della Santina CC, Schubert MC, Minor LB. Disorders of Balance and Vestibular Function in US Adults Data From the National Health and Nutrition Examination Survey, 2001-2004. Arch Intern Med. 2009;169(10):938-944. doi:10.1001/archinternmed.2009.66
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4069154/) - Bergen G, Stevens MR, Burns ER. Falls and Fall Injuries Among Adults Aged ≥65 Years — United States, 2014. MMWR Morb Mortal Wkly Rep 2016;65:993–998. DOI: http://dx.doi.org/10.15585/mmwr.mm6537a2
- Katsarkas A. Nystagmus of paroxysmal positional vertigo: some new insights. Ann Otol Rhinol Laryngol. 1987;96:305–308.
- Oghalai, J. S., et al. (2000). “Unrecognized benign paroxysmal positional vertigo in elderly patients.” Otolaryngol Head Neck Surg 122(5): 630-4
Bio:
Dr. Danielle Gross, PT, DPT (Balance Director)
 Danielle is a doctor of physical therapy who specializes in Vestibular Examination and Rehabilitation, and is the Balance Program Director at FYZICAL Therapy & Balance Center of Rockville. Her passion is to help people who suffer from vestibular dysfunction resolve their symptoms of vertigo, dizziness, and imbalance so that they may regain control of their lives again. She frequently gives presentations in the community to educate and raise awareness about balance and dizziness issues, has created an educational inner ear model, and maintains a blog to serve as an educational resource for the vestibular community at www.Vestibular.Today
Danielle is a doctor of physical therapy who specializes in Vestibular Examination and Rehabilitation, and is the Balance Program Director at FYZICAL Therapy & Balance Center of Rockville. Her passion is to help people who suffer from vestibular dysfunction resolve their symptoms of vertigo, dizziness, and imbalance so that they may regain control of their lives again. She frequently gives presentations in the community to educate and raise awareness about balance and dizziness issues, has created an educational inner ear model, and maintains a blog to serve as an educational resource for the vestibular community at www.Vestibular.Today
FYZICAL Therapy & Balance Center of Rockville
www.FYZICALrockville.com
15201 Shady Grove Road, Suite 106